Natural Choices are indeed better.. especially when proven by science
Milk Calcium, Phosphorus and Vitamin D Tablets


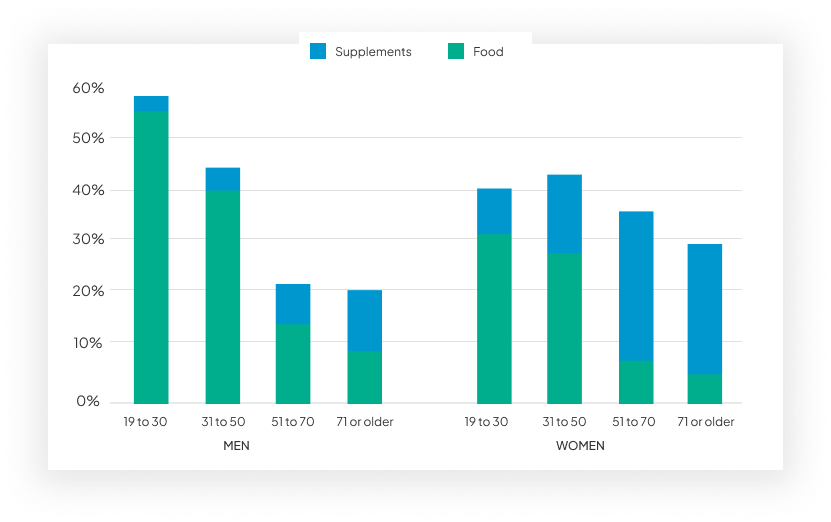
“ 1/3 Women over 50 will experience osteoporotic fractures. As will 1/4 men.”
Worldwide, 1 in 3 women over age 50 will experience osteoporotic fractures, as will 1 in 5 men aged
over 50
By 2050, the worldwide incidence of hip fracture in men is projected to increase by 310% and 240% in
women, compared to rates in 1990.
Mortality rates post-hip fracture vary between 25-30% in western populations, they are 2-3 fold higher
in populations from the Middle East and Africa region.